
What is febrile neutropenia (FN) and why is it an oncologic emergency? 🤒 In Episode 45 of Run the List, Dr. Marlise Luskin (@LuskinMarlise), a hematologist/oncologist🩸at Dana-Farber Cancer Institute breaks it down for us Thanks @OpsBug for covering this week’s topic!
FN is an oncologic emergency w/ 3 major flavors 🍨: 🟣FN w/ isolated pathogen🦠 🔵FN w/ clinical etiology (e.g. cellulitis, pneumonia) 🩺, but w/o isolation of the pathogen 🟡FN w/o clinical etiology nor an identified pathogen (FUO/Fever of Unknown Origin)🤷♂️ FN causes? 👇👇👇

Epidemiological studies 📚✏️ inform us that FN is a significant cause of cancer-related morbidity & mortality Incidence rate? ◾️10-50% for patients w/ solid tumors ◽️≥80% occur in hematologic malignancies (e.g. AML) ◾️Majority of deaths occurring in those aged 65–79

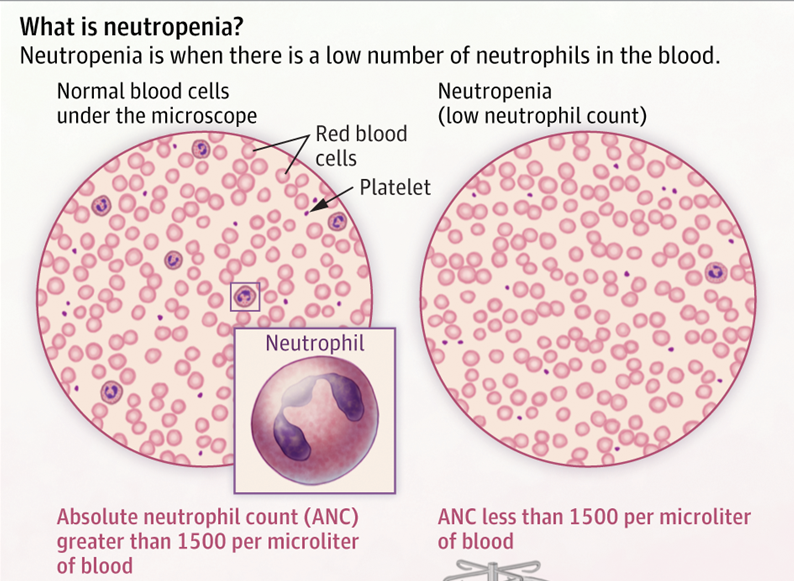
Today's focus: FN in cancer pts 🦀 🔷Dr. Luskin teaches us that fever in FN is defined as temp🌡️> 101, or >100.5 F sustained for an hour ⏰ 🔶Neutropenia is defined as absolute neutrophil count (ANC) <500 cells, occurring w/i 7-12 days in a pt receiving cytotoxic chemotherapy

Empiric therapy for FN was first described in @NEJM by Schimpff et al. (1971) 📝Main focus of abx treatment was Pseudomonas w/ concerns for Gram negative (GN) sepsis🦠 as it carries high mortality Conclusion? 📝1st-line agents must cover GNs & have anti-Pseudomonal activity💊!

⏲️Timely initiation of antibiotics is 🔑 in controlling the underlying infection! 💊Zosyn (piperacillin-tazobactam, anti-Pseudomonal) is a common 1st-line agent But, since resistance is on the rise, keep Carbapenems close 🧐

In the clinic, there's a shift towards 🔍stratifying pts w/ FN between those at high📈 & low📉 risk of septic complications Why? -⌛️Reduces length of hospitalization -🙅♀️Prevents over-treating those at low risk -🎯Targets therapies to an ever-shifting landscape of pathogens 👇

🔍Stratification is done based on presenting signs & symptoms, nature of the underlying malignancy, & existing comorbidities A validated tool 🔨 for accomplishing this is called the: Multinational Association of Supportive Care in Cancer (MASCC) risk index for FN 🧮

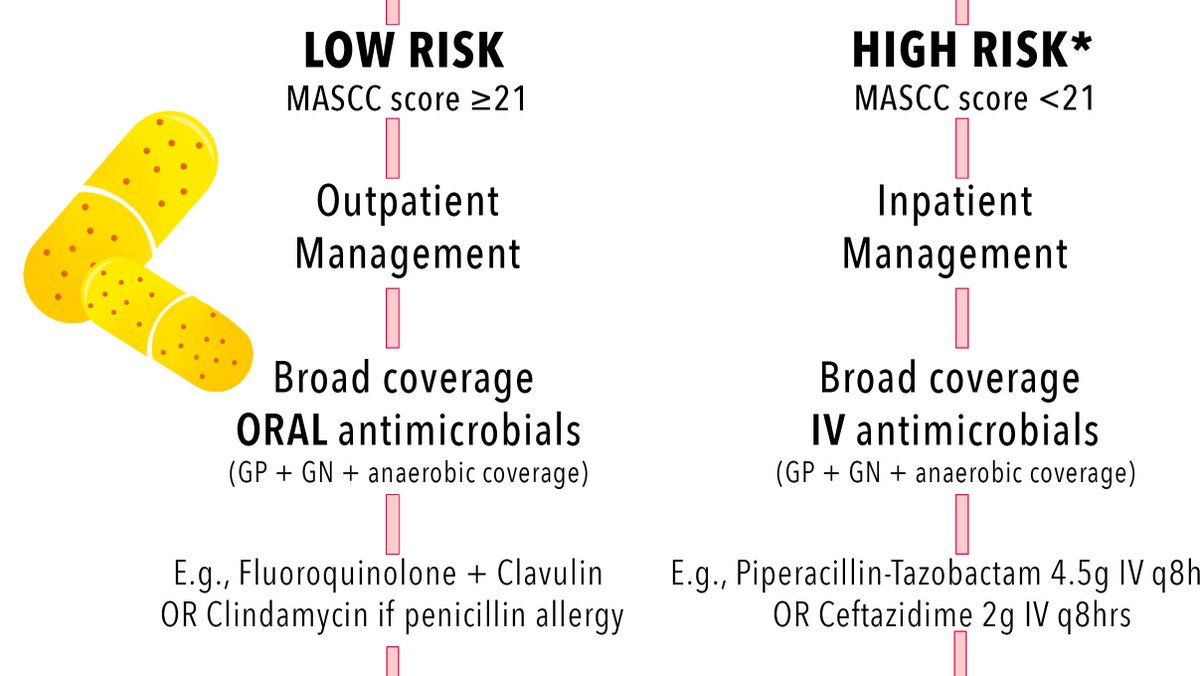
MASCC risk index classifies patients into: -LOW risk (w/ a HIGH score >21) or -HIGH risk (w/ a LOW score <21) These categories carry diagnostic 🩺 relevance: 🔽Low risk pts can be treated outpatient w/ PO abx 💊 🔼High risk pts need to be admitted 🚨 An example 👇
Let's pause for a quick quiz! 🤓 As per MASCC guidelines, can neutropenic fever ever be LOW risk?
However, over time, retrospective studies have shown that low-risk stratification in MASCC score is *not* a sensitive predictor of a pt's clinical status! In a study by Coyne et al. (2016) 👇, MASCC score was only 83% sensitive, & low-risk pts had *more* adverse events 😱
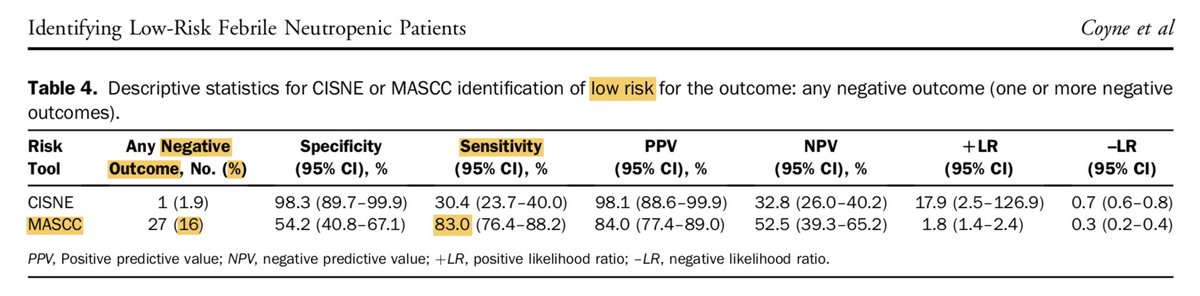
To better capture intermediate-risk events, Coyne et al. devised the Clinical Index of Stable Febrile Neutropenia (CISNE) score 🧮 Compared to MASCC, CISNE does NOT need a subjective assessment of sx severity, requires more historical information, & relies less on acute sx 👇

Ultimately, more sensitive stratification becomes a mechanism for implementing & practicing better 💊antimicrobial stewardship🏆 CISNE calculator: https://t.co/3J6n983ghR - Here’s a #tweetorial from @MayoClinicINFD describing outpatient management of FN: https://t.co/jDOIRqzCoO
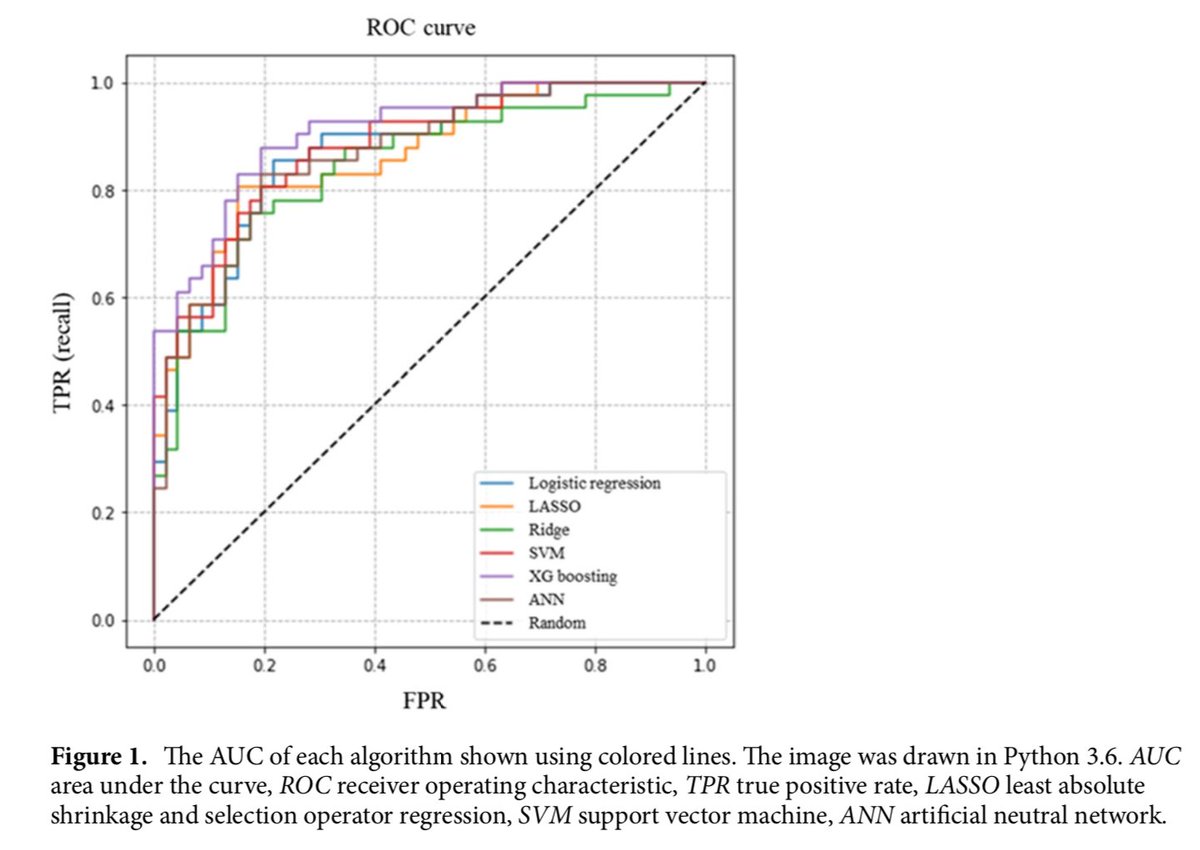
What does the future look like? 👀 🖥️Machine-learning📚 algorithms may be used to improve the prediction of FN in pts undergoing breast cancer chemo tx 🧠Artificial intelligence can tag pts who may be at-risk for FN in the near future but much work remains to be done @EricTopol


Phew! Here are take-home management points for FN: -Have a high index of suspicion in chemo pts -Risk stratify using CISNE > MASCC -Be on lookout for CISNE adoption at your institution! -Start broad spectrum abx w/ Gram negative AND anti-Pseudomonal activity -Place an ID consult

ICYMI: 🎧Listen to RTL Episode 45: Febrile Neutropenia here: https://t.co/XAmOZYJIAs 📝Free download of our 👆-page FN episode handout here: https://t.co/ZtGJ5KhJSk

REFs (1/2): [1]https://t.co/1wAcnvaYTM [2a]https://t.co/wQQLQAEZVj [2b]https://t.co/9bkqmThMuP [3]https://t.co/Yn2e4wu0te [4a]https://t.co/N6YFdtGZKZ [4b]https://t.co/8Lc3sg67va [5]https://t.co/3bMkDgMnvm [6]https://t.co/fZVkNxeKj2 [7]https://t.co/NsAZwV859t
REFs (2/2): [8]https://t.co/9bkqmThMuP [9]https://t.co/8Lc3sg67va [10]https://t.co/QGLpZqTH8E [11, 12, 13]https://t.co/cyBSsYtwUL [14]https://t.co/tCkTks8ydO
@MedTweetorials @CPSolvers @COREIMpodcast @CuriousClinPod @DxRxEdu @rabihmgeha @tony_breu @LuskinMarlise @DavidSteensma